Cardiovascular disease can manifest itself in many forms: high blood pressure, coronary artery disease, valvular disease, stroke, and arrhythmias.
Cardiovascular disease can manifest itself in many forms: high blood pressure, coronary artery disease, valve disease, stroke, and arrhythmias (irregular heartbeats). According to the World Health Organization, cardiovascular diseases cause the death of more than 17 million people in the world each year.
Risk factors are divided into two categories: major and minor. Major risk factors are factors that have been shown to play a role in the risk of cardiovascular disease. Secondary risk factors can increase the risk of these diseases.
The more risk factors a person has, the greater their chances of developing heart disease. Some risk factors can be changed, treated, or modified and others cannot. But controlling as many risk factors as possible, through lifestyle changes and/or medications, can reduce cardiovascular risk.
Main risk factors
High blood pressure (arterial hypertension).
High blood pressure increases your risk of heart disease, heart attack, or stroke. Hypertensive people who are also obese, smoke, or have high blood cholesterol levels have a much higher risk of heart disease or stroke.
Blood pressure can vary depending on the degree of physical activity and age, but normal values for a healthy adult at rest should be 120/80.
High cholesterol.
One of the main cardiovascular risk factors is high cholesterol. Cholesterol, a fatty substance (a lipid) carried in the blood, is found in all cells of the body. The liver produces all the cholesterol the body needs to form cell membranes and produce certain hormones. The body gets extra cholesterol from foods that come from animals (meat, eggs, and dairy products) or that contain large amounts of saturated fat.
When the blood contains too much low-density lipoprotein (LDL, or “bad cholesterol”), it begins to build up on the walls of the arteries, forming plaque and thus starting the disease process called “atherosclerosis.” When plaque builds up in the coronary arteries that supply the heart, there is an increased risk of heart attack.
Diabetes.
Heart problems are the leading cause of death among diabetics, especially those with adult-onset or type II diabetes (also called “non-insulin-dependent diabetes”). Certain racial and ethnic groups (Blacks, Hispanics, Asians, Polynesians, Micronesians, Melanesians, and Amerindians) are at increased risk of diabetes. The American Heart Association (AHA) estimates that 65% of diabetic patients die of some form of cardiovascular disease. If you know you have diabetes, you should be checked by a doctor, because good control of blood glucose (sugar) levels can reduce your cardiovascular risk. If you think you may have diabetes but are not sure, see your doctor who will test you for it.
Obesity and overweight.
Being overweight can raise cholesterol and cause high blood pressure and diabetes. All of these situations are important risk factors for heart disease.
Doctors measure obesity using the Body Mass Index (BMI), which is calculated by dividing the weight in kilograms by the square of the height in meters (BMI = kg/m2). According to the National Lung, Heart, and Blood Institute (NHLBI), a person is considered overweight if they have a BMI greater than 25 and obese if the number is greater than 30. You can determine your BMI using the calculator below. With that number, you can find out your body composition by consulting the table below the calculator.
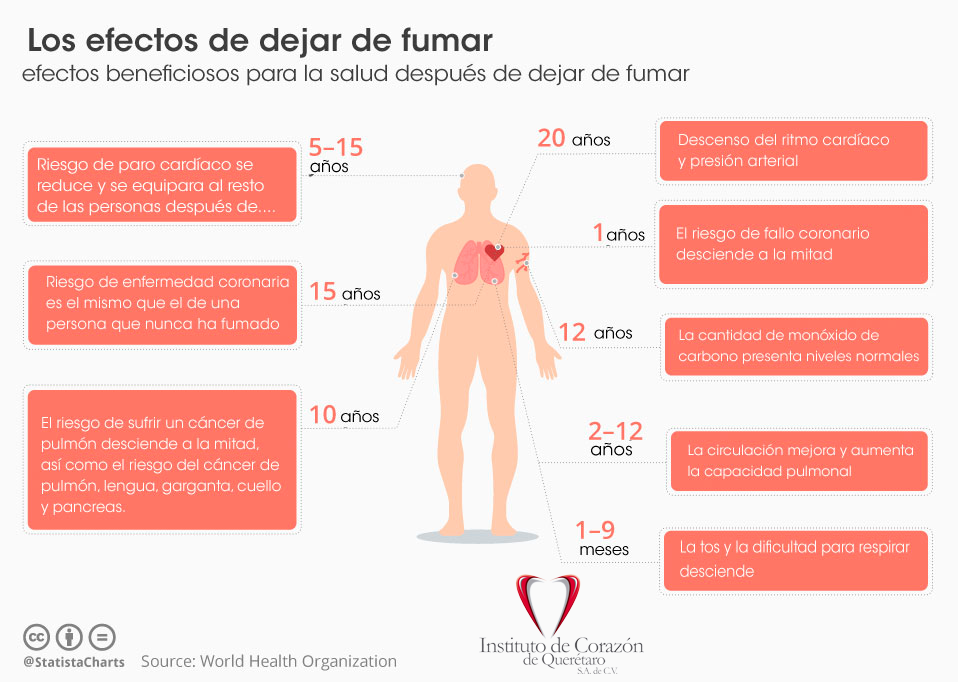
Smoking.
Most people know that smoking increases the risk of lung cancer, but few know that it also significantly increases the risk of cardiovascular disease and peripheral vascular disease (disease of the blood vessels that supply the arms and legs). According to the American Heart Association, more than 400,000 Americans die each year from smoking-related diseases. Many of these deaths are due to the effects of tobacco smoke on the heart and blood vessels.
Smoking raises the heart rate, hardens the large arteries, and can cause heart rhythm irregularities. All of these factors make the heart work harder. In addition, smoking raises blood pressure, which is another important risk factor. Although nicotine is the most important active ingredient in cigarette smoke, other substances and chemicals such as tar and carbon monoxide also damage the heart in many ways.
Physical inactivity.
Inactive people have a higher risk of heart attack than people who exercise regularly. Exercise burns calories to maintain a healthy weight, helps control cholesterol levels and diabetes, and possibly lowers blood pressure. Exercise also strengthens the heart muscle and makes the arteries more flexible. People who actively burn between 500 and 3,500 calories per week, either at work or by exercising, have a longer life expectancy than sedentary people. Even moderate intensity exercise is beneficial if done regularly.
Sex.
In general, men are at higher risk than women for heart attack. The difference is less when women begin menopause, because research shows that estrogen, one of the female hormones, helps protect women from heart disease. But after age 65, cardiovascular risk is about the same in men and women when the other risk factors are similar. Cardiovascular disease affects more women than men, and heart attacks are generally more severe in women than in men.
Inheritance.
Heart disease is usually hereditary. For example, if the parents or siblings had a heart or circulatory problem before the age of 55, the person has a higher cardiovascular risk than someone without such a family history. Risk factors such as high blood pressure, diabetes, and obesity can also be passed from one generation to the next.
Certain forms of cardiovascular disease are more common among certain racial and ethnic groups. For example, studies show that blacks suffer from more severe hypertension and have a higher cardiovascular risk than Caucasians.
Age.
Older people are at higher risk of heart disease. Approximately 4 out of 5 deaths due to heart disease occur in people older than 65 years of age.
With age, the activity of the heart tends to deteriorate. The walls of the heart can become thicker, the arteries can harden and lose their flexibility, and when this happens, the heart cannot pump blood as efficiently as before to the muscles of the body. Due to these changes, cardiovascular risk increases with age. Thanks to their sex hormones, women are generally protected from heart disease until menopause, when their risk begins to increase.
Contributing factors
Stress.
Stress is believed to be a contributing factor to cardiovascular risk. The effects of emotional stress, habits, and socioeconomic status on the risk of heart disease and heart attack are still being studied.
Researchers have discovered several reasons why stress can affect the heart.
Stressful situations increase heart rate and blood pressure, increasing the heart’s need for oxygen.
In times of stress, the nervous system releases more hormones (mainly adrenaline). These hormones increase blood pressure, which can damage the inner lining of the arteries. As artery walls heal, they can harden or thicken, making it easier for plaque to build up.
Stress also increases the concentration of clotting factors in the blood, thus increasing the risk of a clot forming. Clots can totally clog an artery already partially clogged with plaque and lead to a heart attack.
Stress can also contribute to other risk factors. For example, a person suffering from stress may eat more than they should to comfort themselves, may start smoking, or may smoke more than usual.
Sex hormones.
Sex hormones appear to play a role in heart disease. Among women under 40 years of age, it is not common to see cases of heart disease. But between the ages of 40 and 65, when most women go through menopause, a woman’s chances of having a heart attack rise significantly. And, ages 65 and older, women account for about half of all heart attack victims.
Oral contraceptives.
The first birth control pills contained elevated levels of estrogen and progestin, and taking them increased the chances of cardiovascular disease or stroke, especially in women older than 35 who smoked. But today’s oral contraceptives contain much lower doses of hormones and are considered safe in women under 35 years of age who do not smoke or have high blood pressure.
However, oral contraceptives increase the risk of cardiovascular disease and blood clots in women who smoke or have other risk factors, especially if they are older than 35 years. According to the American Heart Association, women taking oral contraceptives should have annual checkups that include monitoring of blood pressure, triglycerides, and blood sugar.
Alcohol.
Studies show that cardiovascular risk is lower in people who drink moderate amounts of alcohol than in people who don’t drink. According to experts, moderate consumption is an average of one or two drinks per day for men and one drink per day for women. A drink is defined as 1.5 fluid ounces (44 ml) of spirits with an alcohol content of 40° (80 proof), 1 fluid ounce (30 ml) of spirits with an alcohol content of 50° (100 proof) , 4 fluid ounces (118 ml) of wine or 12 fluid ounces (355 ml) of beer. But exceeding a moderate alcohol intake can lead to heart-related problems such as high blood pressure, stroke, irregular heartbeat, and cardiomyopathy (heart muscle disease). Also, a typical drink has between 100 and 200 calories. Alcohol calories often increase body fat, which can in turn increase cardiovascular risk. It is not recommended that people who do not drink start drinking or that those who already drink increase their alcohol consumption.
It is never too late or too early to start improving cardiovascular health. Some risk factors can be controlled and others cannot, but by eliminating risk factors that can be changed and properly controlling those that cannot, it is possible to significantly reduce the risk of heart disease.